What is a DRAM?
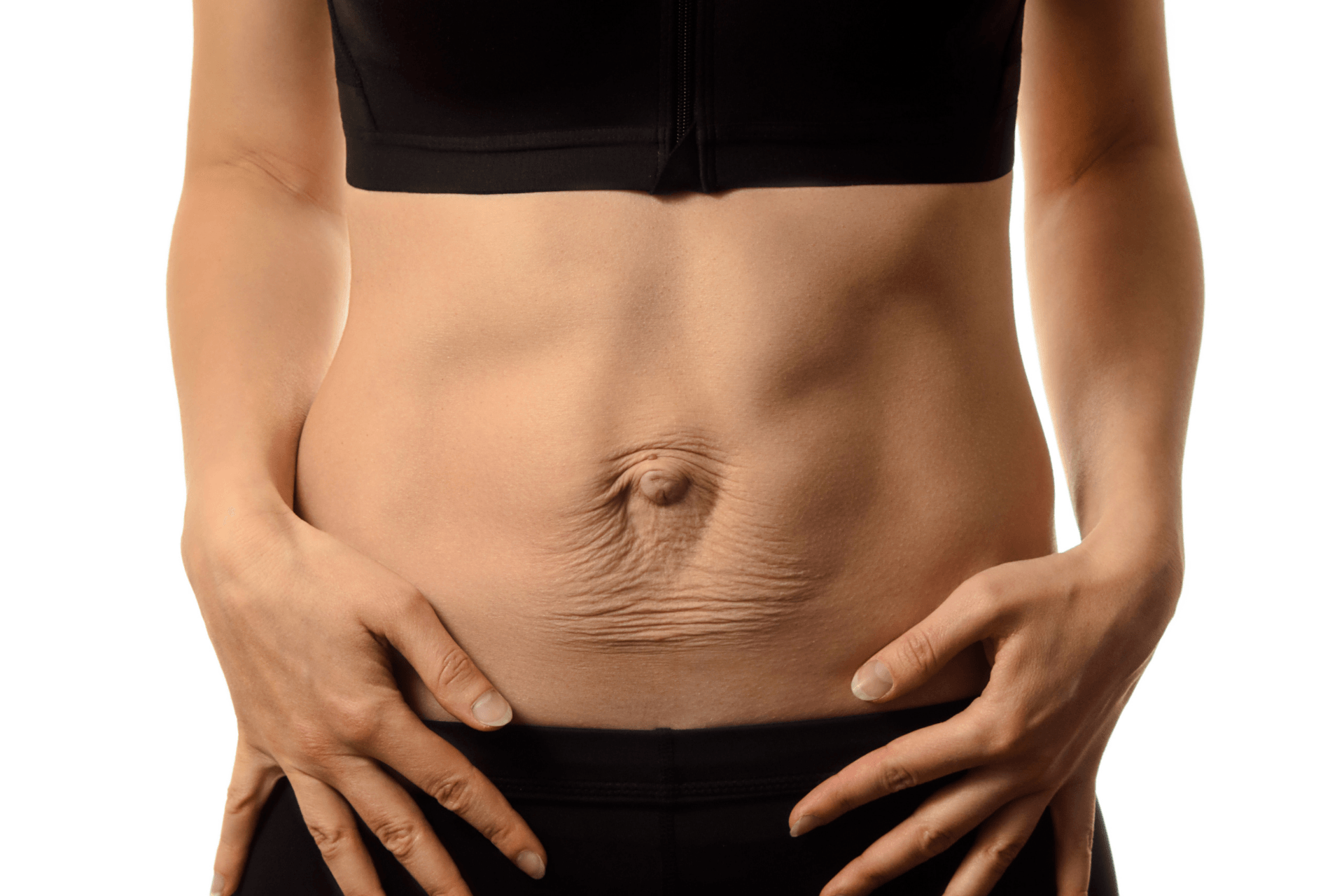
A DRAM (Diastasis Recti) is known as a separation or stretching of the central tendon between your rectus abdominus muscle.
A DRAM is commonly seen in pregnant & postnatal women and can correlate with a large abdominal circumference during pregnancy, a large weight gain, large baby/fluid and weakened abdominal muscles.
During the postnatal period, hormonal changes, increased physical demands and lower abdominal and pelvic floor weakness can all exacerbate the abdominal separation.
Why is important to have my DRAM assessed?
An assessment of your DRAM in the early post natal period will help identify if you have a significant DRAM which places you at increased risk of low back pain, pelvic floor dysfunction, abdominal hernias and other injuries.
A DRAM which is greater than normal width anywhere along your central tendon is clinically significant and requires personalised advice as to safe exercises and or support garments.
How to manage your DRAM
Your Physiotherapist may recommend the following to help in your recovery.
- Compression garments: these will help to provide stability to trunk and lumbar spine, whilst helping to keep your abdominal muscles as close together as possible. Your Physiotherapist will recommend the right garment for you respecting your pelvic floor and stomach stage of recovery.
- Behavioural modification: Learn how to protect your DRAM avoiding activities that increase the strain on the central tendon. Your physiotherapists will ensure you know what to look for that will tell you when you are overloading.
- Safe and effective exercises for you at your stage of recovery respecting pelvic floor.
More from the blog